



With millions of women now taking GLP-1 medications like Ozempic and Wegovy for weight loss, questions about semaglutide and pregnancy have become increasingly common. The short answer? Semaglutide isn’t recommended during pregnancy. But the full picture is more nuanced than a simple “don’t take it.”
This guide covers everything you need to know: what the research actually shows, when to stop if you’re planning pregnancy, what to do if you’ve already been exposed, and how these medications might actually be affecting your fertility in ways you didn’t expect. Whether you’re actively trying to conceive, just discovered you’re pregnant, or simply planning ahead, you’ll find clear guidance here.
Is Semaglutide Safe During Pregnancy?
The straightforward answer is no. Semaglutide is not recommended during pregnancy, and both the FDA and medication manufacturers advise against its use if you’re pregnant or planning to become pregnant.

Here’s why. The FDA states that available data is “insufficient to evaluate for a drug-associated risk of major birth defects, miscarriage, or other maternal or fetal outcomes.” What we do have comes primarily from animal studies, and those findings raised concerns.
When researchers gave semaglutide to pregnant rats at human clinical doses, they observed:
- Increased fetal death
- Structural abnormalities including abnormal heart blood vessels
- Changes in skeletal structures
- Early pregnancy losses in rabbits and cynomolgus monkeys at human-equivalent exposure levels
That said, context matters. Many of these adverse effects coincided with marked maternal body weight loss due to reduced food intake. Some researchers believe the growth issues may be related to weight loss itself rather than the medication directly. We simply don’t have enough human data to separate these factors clearly.
Beyond the direct medication concerns, there’s another fundamental issue. Doctors don’t recommend intentional weight loss during pregnancy, period. Semaglutide works by reducing appetite and food intake. That mechanism, regardless of the drug itself, isn’t appropriate when you’re growing a baby.
The Australian Therapeutic Goods Administration (TGA) classifies semaglutide as a Category D medication for pregnancy, meaning there’s evidence of human fetal risk but the benefits may still outweigh risks in certain situations (like poorly controlled diabetes).
| Medication | Pregnancy Category | Recommended Washout Period |
|---|---|---|
| Semaglutide (Ozempic, Wegovy) | Category D (TGA) | 2 months before conception |
| Tirzepatide (Mounjaro, Zepbound) | Not formally assigned | 1 month before conception |
| Liraglutide (Saxenda, Victoza) | Category C | Shorter half-life; discuss with provider |
For women using compounded semaglutide or brand-name versions, the guidance remains the same: discontinue before pregnancy and use reliable contraception while taking the medication.
What the Research Actually Shows
Most of our safety data comes from animal studies, which isn’t unusual. It’s not ethical to conduct medication trials on pregnant humans, so researchers rely on animal models and observational data from accidental exposures.
The animal findings were concerning. Pregnant rats given semaglutide at clinically relevant doses produced offspring with reduced growth and increased skeletal and visceral malformations. Pregnant cynomolgus monkeys showed more frequent early pregnancy losses. These findings are why the FDA includes pregnancy warnings on all semaglutide products.
But here’s what’s encouraging. Human data, while limited, has been more reassuring than the animal studies might suggest.
A 2025 study published in Basic & Clinical Pharmacology & Toxicology examined 32 pregnancies exposed to semaglutide alongside insulin. The researchers found comparable risks of malformations, preterm birth, and neonatal complications compared to pregnancies exposed only to insulin. That’s a small sample, but it’s meaningful.
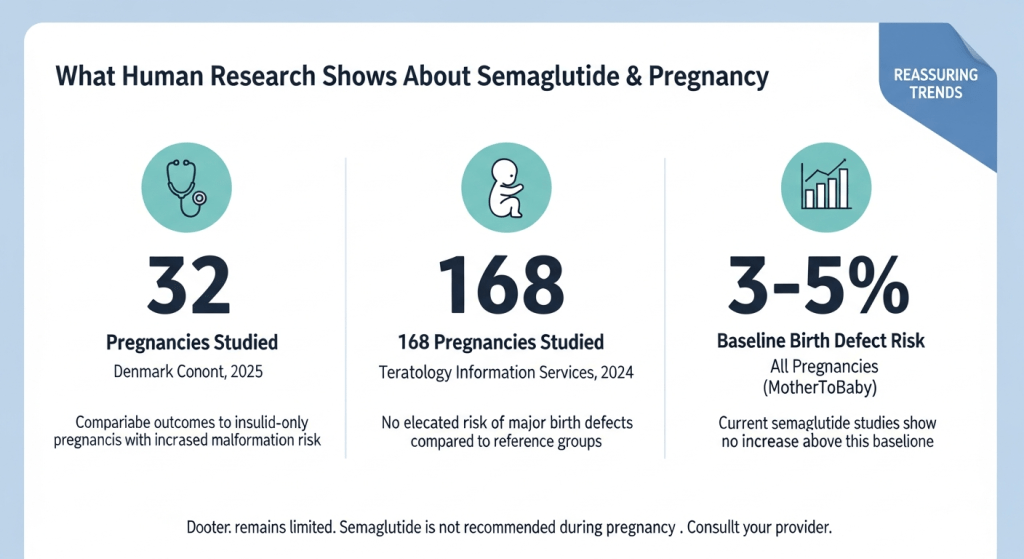
A larger multicenter observational study from the Teratology Information Services analyzed 168 pregnancies with first-trimester GLP-1 exposure. They compared outcomes to two reference groups: women with diabetes on other medications and overweight/obese women without diabetes. The study did not find an elevated risk of major birth defects associated with GLP-1 use.
What does this mean for you? The absence of human studies showing clear harm is reassuring, but it’s not the same as proof of safety. Given the current knowledge gaps, the recommendation against use during pregnancy remains appropriate. If you’ve had accidental exposure, though, the available data suggests outcomes are often positive.
When to Stop Semaglutide Before Getting Pregnant
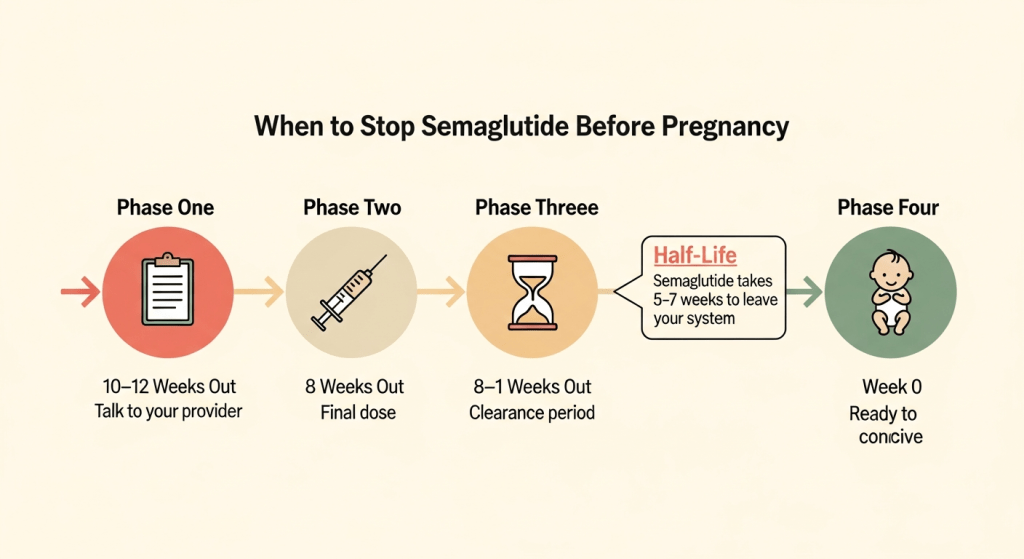
If you’re planning pregnancy, timing matters. The FDA and medication manufacturers recommend stopping semaglutide at least two months before you start trying to conceive.
Why two months? It comes down to pharmacokinetics. Semaglutide has a long half-life of about one week, meaning it takes 5 to 7 weeks for the medication to fully clear your system after your last dose. The two-month recommendation builds in a safety buffer.
Here’s a practical timeline if you’re planning pregnancy:
- 10-12 weeks before trying to conceive: Talk with your healthcare provider about your pregnancy plans and discuss transitioning off semaglutide.
- 8 weeks before: Take your final semaglutide dose.
- 8 weeks to conception: Allow full medication clearance. Focus on maintaining healthy habits (nutrition, exercise, sleep) that support both weight maintenance and fertility.
- When actively trying: You should be fully clear of semaglutide. If conception takes longer than expected, you’ll already be medication-free.
Some providers may suggest switching to liraglutide (Saxenda or Victoza) if you need to continue GLP-1 therapy closer to conception. Liraglutide is taken daily rather than weekly, so it doesn’t remain in your system as long and can be stopped closer to when you begin trying.
One thing to be aware of: stopping semaglutide can affect your fertility in an unexpected way. Many women experience improved ovulation and fertility after weight loss on GLP-1 medications. If you’ve been relying on irregular cycles as informal birth control, that may no longer work once you’ve lost weight. Use reliable contraception until you’re ready.
Working with a provider who understands both weight management and reproductive health makes this transition smoother. Your provider can help you maintain your progress while preparing your body for pregnancy.
What If You Got Pregnant While Taking Semaglutide?
First, don’t panic. This situation is more common than you might think, and the outcomes are generally encouraging.
If you discover you’re pregnant while on semaglutide, here’s what to do:
- Stop the medication immediately. There’s no need to taper. Simply discontinue your next scheduled dose and contact your healthcare provider.
- Notify your OB-GYN or midwife. Let them know when you took your last dose and how long you were on the medication. This information helps them plan appropriate monitoring.
- Understand that early exposure often has good outcomes. The limited human data we have shows that most pregnancies with first-trimester semaglutide exposure result in healthy babies.
- Expect standard prenatal monitoring. Your provider may recommend additional ultrasounds to monitor fetal development, but this is precautionary rather than cause for alarm.
Experts note that every pregnancy starts with a 3-5% baseline chance of birth defects regardless of medication exposure. Current research hasn’t clearly demonstrated that semaglutide increases this baseline risk in humans.
But what if you took semaglutide before you knew you were pregnant? This is the most common scenario, and it’s exactly why researchers have been studying early exposure outcomes. The studies suggest that inadvertent first-trimester exposure doesn’t appear to dramatically increase risks compared to other diabetes medications.
If you have diabetes and were taking semaglutide for blood sugar control, the conversation with your provider becomes more nuanced. Uncontrolled blood sugar during pregnancy carries its own serious risks for birth defects and complications. Your provider will help weigh the risks of medication exposure against the risks of poorly controlled diabetes.
Semaglutide, Fertility, and “Ozempic Babies”
You may have heard the term “Ozempic babies” floating around social media. It refers to unexpected pregnancies among women taking GLP-1 medications who didn’t think they could conceive easily.
Here’s what’s actually happening. Semaglutide isn’t a fertility medication. It doesn’t directly enhance your ability to get pregnant. But the weight loss it produces can have significant effects on reproductive function.

For women with obesity, excess weight often disrupts hormonal balance and ovulation. Conditions like polycystic ovary syndrome (PCOS) are strongly linked to insulin resistance and weight. When women lose significant weight on GLP-1 medications, several things can happen:
- Ovulation may resume or become more regular
- Menstrual cycles that were previously irregular may normalize
- Hormonal imbalances that were suppressing fertility may correct themselves
The result? Women who assumed they couldn’t get pregnant (or who were relying on irregular cycles as informal birth control) suddenly find themselves with a positive pregnancy test.
This isn’t a side effect of the medication itself. It’s a consequence of the metabolic improvements that come with weight loss. But it catches many women off guard.
If you’re taking semaglutide and don’t want to become pregnant, use reliable contraception. The medication may also reduce the effectiveness of oral birth control pills due to delayed gastric emptying, so adding a barrier method is wise.
If you’re taking semaglutide specifically to improve fertility (some providers prescribe it off-label for PCOS-related infertility), work closely with your healthcare team on timing. You’ll want to achieve your weight loss goals, then transition off the medication before actively trying to conceive.
The FDA emphasizes that women of childbearing potential should use contraception during semaglutide therapy.
Can You Take Semaglutide While Breastfeeding?
The guidance here is less clear-cut than for pregnancy, and it depends on which form of semaglutide you’re considering.
For injectable semaglutide (Ozempic, Wegovy):
The situation is somewhat reassuring. According to MotherToBaby, a small study of 8 breastfeeding women taking up to 1.0 mg weekly found that semaglutide was not detectable in their breastmilk samples. The medication’s large molecular size makes it unlikely to pass into milk in significant amounts, and even if it did, it would probably be destroyed in the infant’s digestive tract.
For oral semaglutide (Rybelsus):
This is a different story. The tablet contains an absorption enhancer called salcaprozate sodium (SNAC) that helps the medication get absorbed in your gut. This compound has been found in concentrated amounts in the milk of lactating rats. Because infants have lower levels of the enzyme needed to clear SNAC, there’s theoretical concern about accumulation in breastfed babies. For this reason, the product label for Rybelsus specifically recommends against use while breastfeeding.
Most authorities recommend caution with any semaglutide use during breastfeeding simply because we don’t have robust human data. The developmental benefits of breastfeeding need to be weighed against any potential risks from medication exposure.
Talk with your baby’s pediatrician and your own healthcare provider before making this decision. Many women choose to wait until they’ve finished breastfeeding before resuming GLP-1 medications.
What About Rebound Weight Gain?
This is often the unspoken concern. You’ve worked hard to lose weight on semaglutide. Now you need to stop for pregnancy. Will you gain it all back?
The honest answer: weight regain after stopping GLP-1 medications is common. Research shows that without the appetite-suppressing effects of semaglutide, many people gradually return toward their previous weight.
One case report published in the International Journal of Gynecology & Obstetrics documented a woman who stopped semaglutide early in pregnancy and experienced significant weight gain not just in the third trimester but throughout her entire pregnancy. The researchers suspected this was partly rebound weight gain from discontinuing the medication.
But here’s some important context. Weight gain during pregnancy is normal and necessary. The goal isn’t to maintain your pre-pregnancy weight; it’s to gain an appropriate amount for a healthy pregnancy.
Current guidelines suggest:
- Women with normal BMI: gain 25-35 pounds
- Women who are overweight: gain 15-25 pounds
- Women with obesity: gain 11-20 pounds
Strategies to minimize excessive weight gain after stopping semaglutide:
- Transition gradually if possible. Work with your provider to time your discontinuation thoughtfully rather than stopping abruptly at the moment you discover pregnancy.
- Maintain the habits you built. The behaviors you developed while on semaglutide (portion awareness, reduced snacking, increased protein intake) can continue without the medication. A focus on balanced nutrition becomes even more important during this transition.
- Stay active. Regular physical activity during pregnancy supports healthy weight gain and makes it easier to return to your goals postpartum.
- Plan for the future. You can resume semaglutide after pregnancy and breastfeeding are complete. Many women successfully return to their weight loss goals when the time is right.
Minimal’s care team can help you create a transition plan that accounts for both your health goals and your pregnancy plans. Having a provider who understands weight management makes navigating this transition much smoother.
Check your eligibility to speak with a Minimal provider about your specific situation.

Summing Up:
The relationship between semaglutide and pregnancy comes down to timing and planning. While this medication isn’t appropriate during pregnancy, millions of women have successfully navigated the transition from weight loss treatment to healthy pregnancies.
If you’re currently on semaglutide and thinking about pregnancy, now is the time to have that conversation with your healthcare provider. Creating a transition plan well in advance gives you the best chance of protecting both your health goals and your future pregnancy.
And if you’ve already discovered you’re pregnant while on semaglutide, the available research suggests reason for cautious optimism. Stop the medication, connect with your prenatal provider, and focus on the healthy pregnancy ahead.
FAQs
What happens if you get pregnant while taking semaglutide?
If you discover you’re pregnant while on semaglutide, stop taking it immediately and contact your healthcare provider. There’s no need to panic. While semaglutide isn’t recommended during pregnancy due to concerning animal study findings, human data has been more reassuring. The Denmark cohort study found that women exposed to semaglutide in early pregnancy had comparable outcomes to those on insulin alone. Your provider will likely schedule additional ultrasounds to monitor fetal development, but this is precautionary. The most important step is discontinuing the medication promptly and beginning appropriate prenatal care.
Should I stop taking semaglutide if I’m pregnant?
Yes, you should stop semaglutide as soon as you confirm pregnancy. The FDA and all medication manufacturers recommend discontinuing semaglutide when pregnancy is recognized. There’s no need to taper off gradually. Simply skip your next scheduled dose and notify your OB-GYN or midwife about when you took your last injection and how long you were on the medication. This information helps your care team plan any additional monitoring that may be appropriate for your situation.
What are the birth defects of semaglutide?
In animal studies, semaglutide exposure during pregnancy was associated with structural abnormalities including cardiovascular malformations, skeletal variations, and reduced fetal growth. However, many of these effects occurred at doses that also caused significant maternal weight loss, making it difficult to determine whether the medication itself or the weight loss caused the problems. Human data tells a different story. Studies examining over 200 pregnancies with first-trimester GLP-1 exposure have not found elevated rates of major birth defects compared to other diabetes medications. Every pregnancy carries a 3-5% baseline risk of birth defects regardless of medication exposure.
How long do I have to be off Ozempic before getting pregnant?
The manufacturer recommends stopping Ozempic at least two months before attempting to conceive. This timeframe accounts for the medication’s long half-life and provides a safety buffer to ensure semaglutide has fully cleared your system before conception occurs. If you’re planning pregnancy, talk with your healthcare provider about creating a transition plan that includes timing your final dose.
How long does semaglutide stay in your system?
Semaglutide has a half-life of approximately one week, which is why it’s dosed weekly rather than daily. After your last injection, it takes about 5 to 7 weeks for the medication to be eliminated from your body. This extended clearance time is why the two-month pre-conception recommendation exists. The medication continues working during this washout period, so you may still experience appetite suppression and weight management effects for several weeks after your final dose.









